PAH Patients Can Be at Greater Risk Than They Present1-3
Findings from the Reveals Registry*
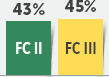
Clinical worsening of PAH within 1 year was reported to be 43% in FC II patients (401/925) and 45% in FC III patients (625/1399)1†
In an additional analysis of first-time hospitalizations, almost 1 in 4 (24% [58/244]) of PAH-related hospitalizations occurred in newly diagnosed FC II patients2‡
of PAH-related hospitalizations (136/244) occurred in newly diagnosed FC III patients2‡
REVEAL was a US-based, observational registry involving 55 academic- and community-based treatment centers. 3515 patients enrolled between March 2006 and December 2009.4
*REVEAL (Registry to Evaluate Early and Long-term PAH Disease Management) was funded and sponsored by Actelion Pharmaceuticals US, Inc.4
†Analysis included 3001 patients. The analysis criteria included patients age >18 years with PCWP ≤15 mmHg at diagnostic RHC. Clinical worsening was defined as worsening NYHA FC, a ≥15% reduction in 6MWD, all-cause hospitalization, or the introduction of a parenteral prostacyclin analog for any reason. Excludes patients who died or had a major event without a worsening event.
‡Newly diagnosed defined as within 90 days of registry enrollment. Analysis evaluated 862 newly diagnosed patients for first-time hospitalization. Hospitalizations were categorized as PAH related or PAH unrelated based on case report forms. Categories were defined prior to independent review. Of the 862 patients, 257 were hospitalized for PAH, of which 244 patients had available FC assessment. Data shown represent patients with a PAH-related hospitalization and FC assessment.
6MWD=6-minute walk distance; FC=Functional Class; NYHA=New York Heart Association; PCWP=pulmonary capillary wedge pressure; RHC=right heart catheterization.
References:1. Frost AE, Badesch DB, Miller DP, et al. Evaluation of the predictive value of a clinical worsening definition using 2-year outcomes in patients with pulmonary arterial hypertension: a REVEAL Registry analysis. CHEST. 2013;144(5):1521-1529. 2. Burger CD, Long PK, Shah MR, et al. Characterization of first-time hospitalizations in patients with newly diagnosed pulmonary arterial hypertension in the REVEAL Registry. CHEST. 2014;146(5):1263-1273. 3. Humbert M, Kovacs G, Hoeper MM, et al; ESC/ERS Scientific Document Group. 2022 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS). Eur Heart J. 2022;43(38):3618-3731. 4. McGoon MD, Miller DP. REVEAL: a contemporary US pulmonary arterial hypertension registry. Eur Respir Rev. 2012;21(123):8-18.
This site is intended for U.S. healthcare professionals
Clicking continue below will take you to the selected site, the content for which Janssen is not responsible and to which this Privacy Policy does not apply. We encourage you to read the Privacy Policy of every online service you visit.
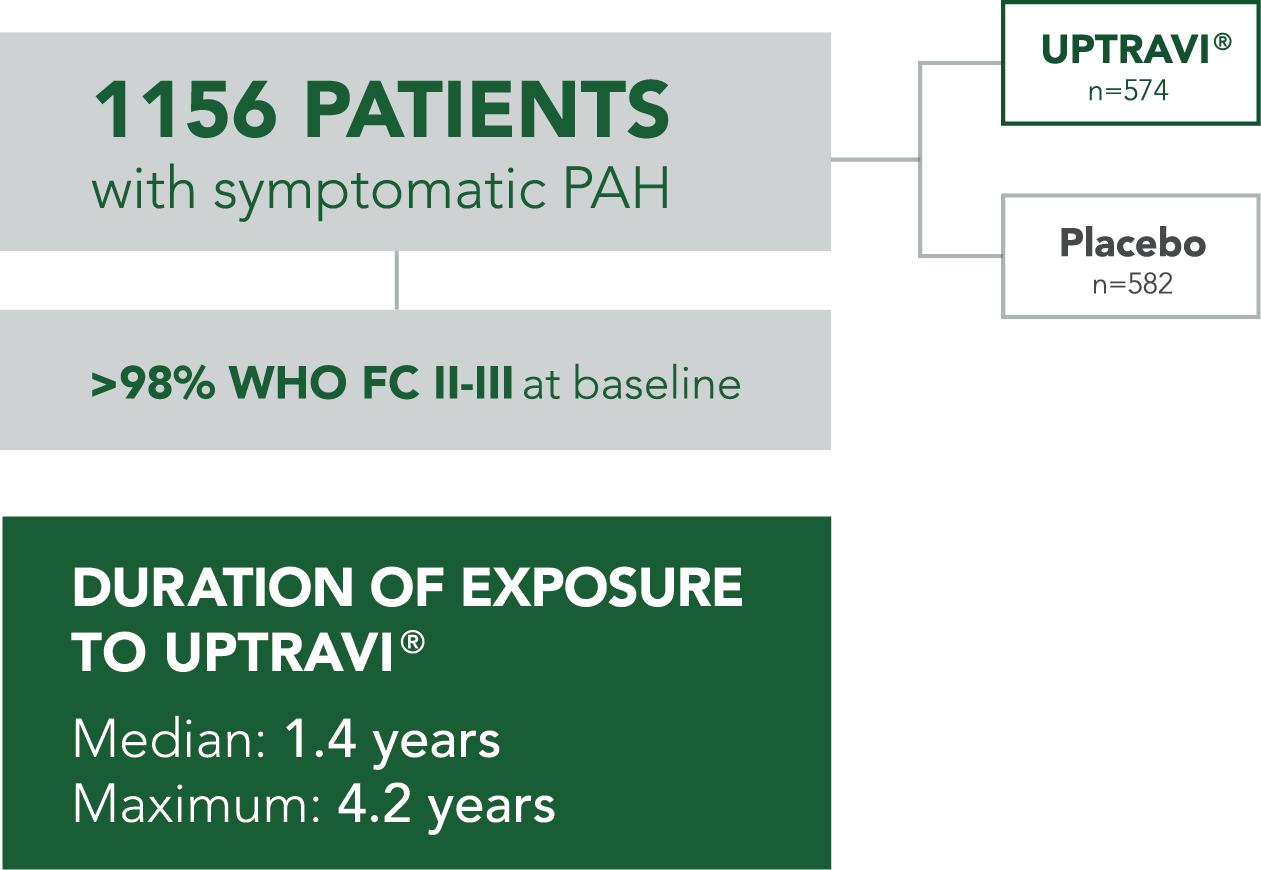
After the starting dose of 200 mcg twice daily, all patients completed titration to their maintenance dose within the first 12 weeks, up to a maximum dose of 1600 mcg twice daily.
Primary endpoint: time to first PAH disease progression event
Death
Hospitalization for PAH
Need for lung transplantation or balloon atrial septostomy for worsening of PAH
Parenteral prostanoid or chronic oxygen therapy
Other disease progression (decrease in 6MWD plus worsening of FC or need for other therapy)
Baseline patient characteristics
Mean age: 48 years
Female: 80%
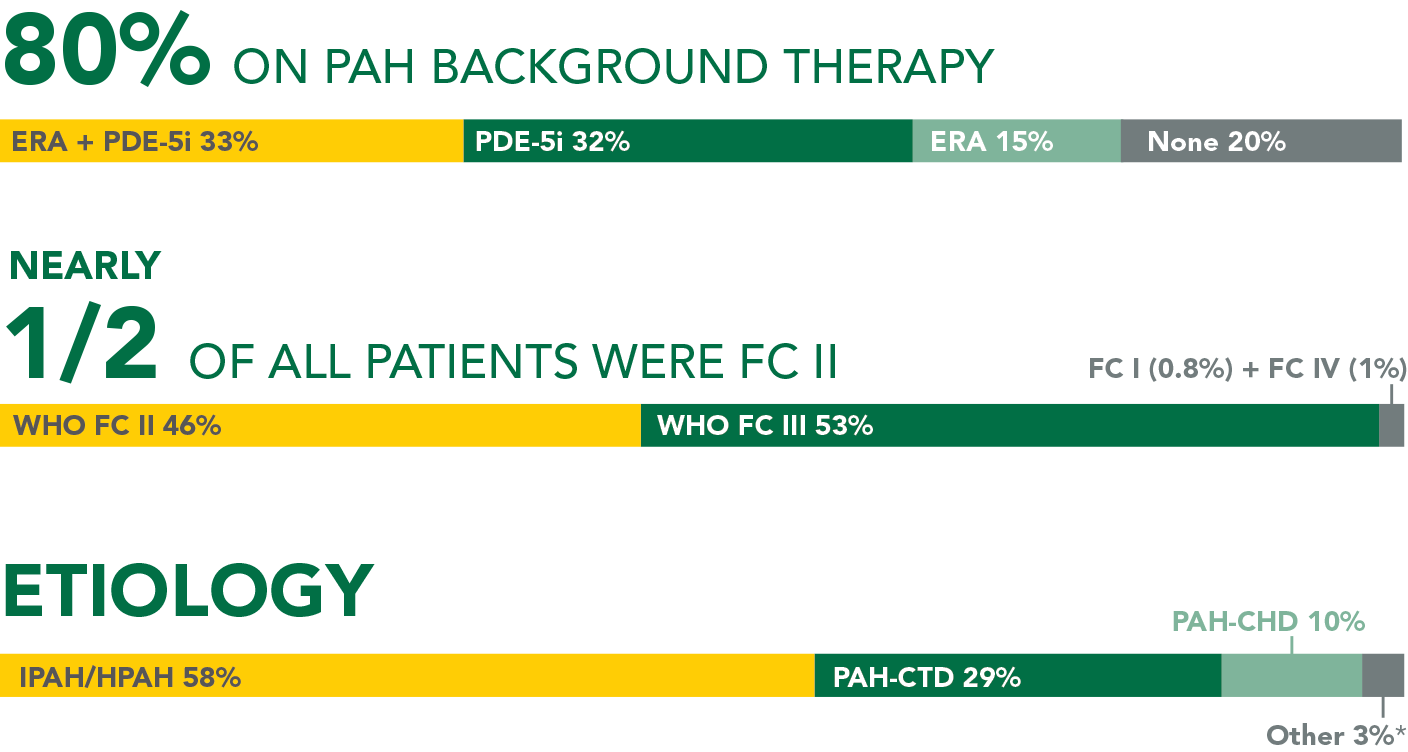
*Other=drugs and toxins (2%) and HIV (1%).
6MWD=6-minute walk distance; ERA=endothelin receptor antagonist; FC=Functional Class; GRIPHON=Prostacyclin (PGI2) Receptor Agonist In Pulmonary Arterial HypertensiON; HIV=human immunodeficiency virus; HPAH=heritable PAH; IPAH=idiopathic PAH; PAH-CHD=PAH associated with congenital heart disease with repaired shunts; PAH-CTD=PAH associated with connective tissue disease; PDE-5i=phosphodiesterase type-5 inhibitor; WHO=World Health Organization.
References: 1. UPTRAVI® (selexipag) full Prescribing Information. Actelion Pharmaceuticals US, Inc. 2. Ruopp NF, Cockrill BA. Diagnosis and treatment of pulmonary arterial hypertension: a review. JAMA. 2022;327(14):1379-1391. 3. Sitbon O, Channick R, Chin KM, et al. Selexipag for the treatment of pulmonary arterial hypertension. N Engl J Med. 2015;373:2522-2533. 4. Coghlan JG, Channick R, Chin K, et al. Targeting the prostacyclin pathway with selexipag in patients with pulmonary arterial hypertension receiving double combination therapy: insights from the randomized controlled GRIPHON study. Am J Cardiovasc Drugs. 2018;18(1):37-47.
UPTRAVI® WAS STUDIED IN GRIPHON, A LARGE OUTCOMES TRIAL IN PAH (N=1156)1
After the starting dose of 200 mcg twice daily, all patients completed titration to their maintenance dose within the first 12 weeks, up to a maximum dose of 1600 mcg twice daily.
Primary endpoint: time to first PAH disease progression event
Death
Hospitalization for PAH
Need for lung transplantation or balloon atrial septostomy for worsening of PAH
Parenteral prostanoid or chronic oxygen therapy
Other disease progression (decrease in 6MWD plus worsening of FC or need for other therapy)
Baseline patient characteristics
Mean age: 48 years
Female: 80%
*Other=drugs and toxins (2%) and HIV (1%).
6MWD=6-minute walk distance; ERA=endothelin receptor antagonist; FC=Functional Class; GRIPHON=Prostacyclin (PGI2) Receptor Agonist In Pulmonary Arterial HypertensiON; HIV=human immunodeficiency virus; HPAH=heritable PAH; IPAH=idiopathic PAH; PAH-CHD=PAH associated with congenital heart disease with repaired shunts; PAH-CTD=PAH associated with connective tissue disease; PDE-5i=phosphodiesterase type-5 inhibitor; WHO=World Health Organization.
Reference: 1. UPTRAVI® (selexipag) full Prescribing Information. Actelion Pharmaceuticals US, Inc.